- info@siyaramhospitals.com
- Tikait Nagar, Uttar Pradesh 225415
- We’re Open 24/7 – Ready to Serve You Anytime
Notice: Our emergency department now offers 24/7 specialized care with reduced wait times. View Emergency Protocols
Insta Gallery






Notice: Our emergency department now offers 24/7 specialized care with reduced wait times. View Emergency Protocols
Gentle & Effective Healing at Siyaram Hospital
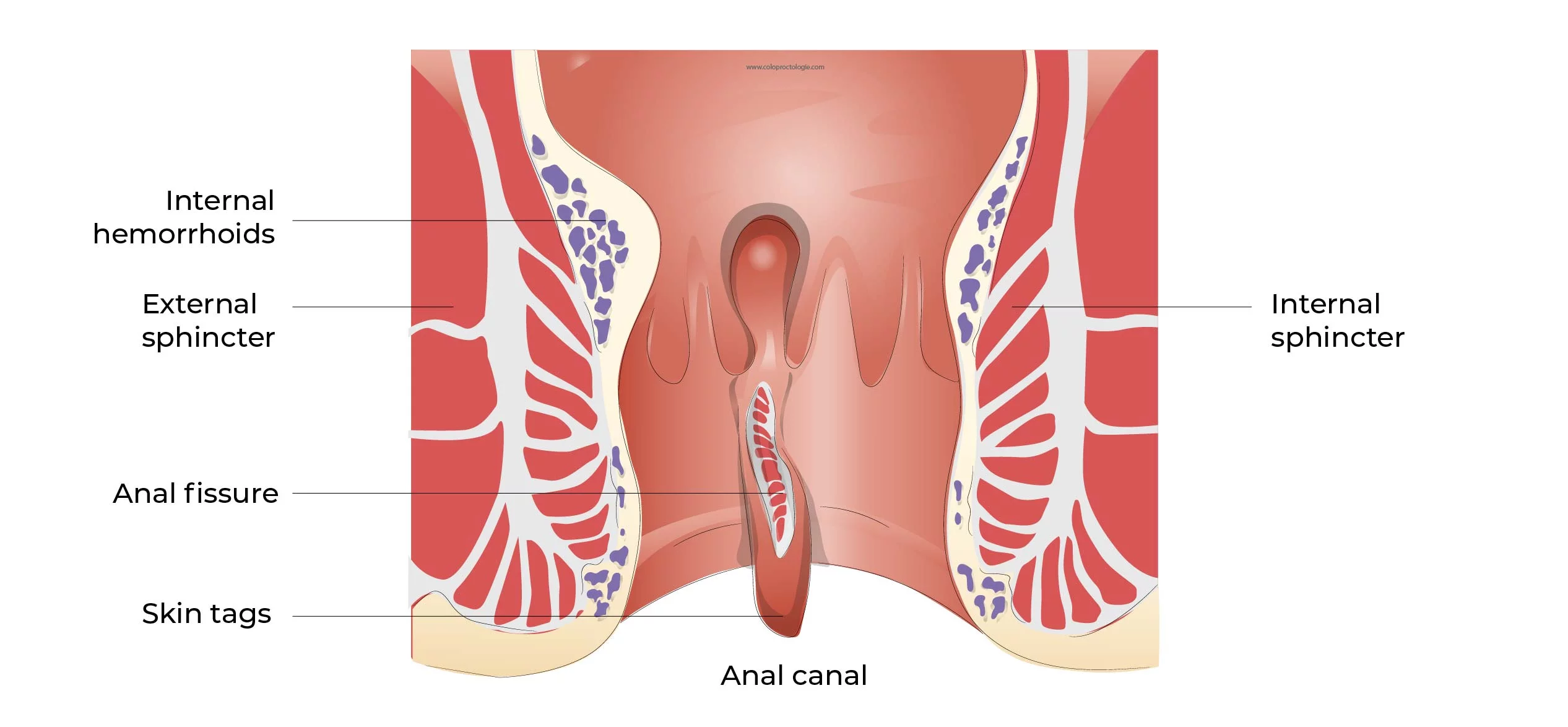
An anal fissure is a small tear in the lining of the anus that causes sharp pain and occasional bleeding during bowel movements. At Siyaram Hospital, we specialize in non-surgical and minimally invasive treatments that help heal fissures effectively, restoring comfort and peace of mind.
Our specialists conduct a gentle physical examination and may perform a digital rectal exam. In some cases, an anoscopy (a small, lighted scope) is used for a closer look. If the area is too painful, a topical anesthetic is applied to keep you comfortable during the diagnosis.
Lidocaine ointment is applied to numb the area before passing stool. This provides fast relief and helps the fissure start healing.
Glyceryl trinitrate (GTN) helps relax the muscle and increase blood flow to promote healing. Applied directly twice daily.
For patients who can’t use GTN, these medicines relax the muscle and reduce pain and spasms effectively.
A modern solution for chronic fissures. Botox helps relax the sphincter muscle and allows the tear to heal naturally.
Most fissures heal within 4–8 weeks with proper care. At Siyaram Hospital, we recommend staying hydrated, eating a fiber-rich diet, and using stool softeners if needed. Our care team provides clear aftercare instructions to minimize discomfort and ensure faster recovery.
Speak with our team at Siyaram Hospital today. Fast, confidential advice is just a click away.
Chat on WhatsApp