- contact@siyaramhospitals.com
- By-Pass Road, Tikait Nagar, Uttar Pradesh 225415
- Open 24/7 for all your healthcare needs
Notice: For Emergencies, please call +91-8381308083. Our team available to assist you 24/7.Get More Info
Gallery Posts






Notice: For Emergencies, please call +91-8381308083. Our team available to assist you 24/7.Get More Info
At Siyaram Hospital, we provide personalized medical solutions to enhance patient health and well-being, delivered by skilled professionals using advanced medical technology.
| Mon - Fri: | 8:00 am - 8:00 pm |
| Saturday: | 9:00 am - 6:00 pm |
| Sunday: | 9:00 am - 6:00 pm |
Hemorrhoid’s are swollen blood vessels in or around the anus and rectum. The haemorrhoidal veins are located in the lowest part of the rectum and the anus. Sometimes they swell so that the vein walls become stretched, thin, and irritated by passing bowel movements. Haemorrhoids are classified into two general categories: internal and external.
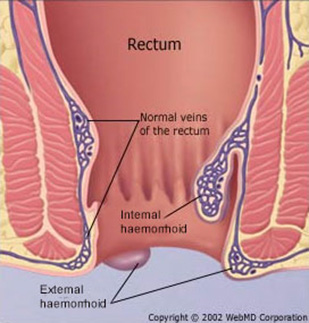
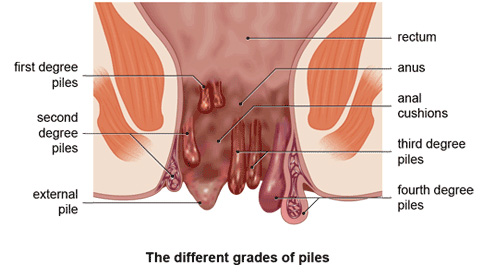
Internal haemorrhoids lie far enough inside the rectum that you can’t see or feel them. They don’t usually hurt because there are few pain-sensing nerves in the rectum. Bleeding may be the only sign that they are there. Sometimes internal haemorrhoids prolapse, or enlarge and protrude outside the anal sphincter. If so, you may be able to see or feel them as moist, pink pads of skin that are pinker than the surrounding area. Prolapsed hemorrhoid’s may hurt because they become irritated by rubbing from clothing and sitting. They usually recede into the rectum on their own; if they don’t, they can be gently pushed back into place.
External haemorrhoids lie within the anus and are often uncomfortable. If an external haemorrhoid prolapses to the outside (usually in the course of passing a stool), you can see and feel it. Blood clots sometimes form within prolapsed external haemorrhoids, causing an extremely painful condition called a thrombosis. If an external haemorrhoid becomes thrombosed, it can look rather frightening, turning purple or blue, and could possibly bleed. Despite their appearance, thrombosed haemorrhoids are usually not serious and will resolve themselves in about a week. If the pain is unbearable, the thrombosed haemorrhoid can be removed with surgery, which stops the pain.
Anal bleeding and pain of any sort is alarming and should be evaluated; it can indicate a life-threatening condition, such as colorectal cancer. Haemorrhoids are the main cause of anal bleeding and are rarely dangerous, but a definite diagnosis from your doctor is essential.
Anyone at any age can be affected by haemorrhoids. They are very common, with about 50% of people experiencing them at some time in their life. However, they are usually more common in elderly people and during pregnancy. Researchers are not certain what causes haemorrhoids. “Weak” veins – leading to haemorrhoids and other varicose veins – may be inherited.
It’s likely that extreme abdominal pressure causes the veins to swell and become susceptible to irritation. The pressure can be caused by obesity, pregnancy, standing or sitting for long periods, straining on the toilet, coughing, sneezing, vomiting, and holding your breath while straining to do physical labour.
Diet has a pivotal role in causing – and preventing – haemorrhoids. People who consistently eat a high-fibre diet are less likely to get haemorrhoids, but those who prefer a diet high in processed foods are at greater risk of haemorrhoids. A low-fibre diet or inadequate fluid intake can cause constipation, which can contribute to haemorrhoids in two ways: it promotes straining on the toilet and it also aggravates the haemorrhoids by producing hard stools that further irritate the swollen veins.
The symptoms of haemorrhoids include:
First, your doctor will look at the anal area, perhaps by inserting a lubricated gloved finger or an anoscope (a hollow, lighted tube for viewing the lower few inches of the rectum) or a proctoscope (which works like an anoscope, but provides a more thorough rectal examination).
More procedures may be needed to identify internal haemorrhoids or rule out other ailments that frequently cause anal bleeding, such as anal fissure, colitis, Crohn’s disease, and colorectal cancer.
To see further into the anal canal (into the lower, or sigmoid, colon), sigmoidoscopy may be used, or the entire colon may be viewed with colonoscopy. For both procedures, a lighted, flexible viewing tube is inserted into the rectum. A barium X-ray can show the entire colon’s interior. First a barium enema is given and then X-rays are taken of the lower gastrointestinal tract.
There are treatments for piles available from pharmacies or through a GP.
Creams, ointments and suppositories can help relieve swelling and inflammation symptoms in the short term. A GP may recommend corticosteroid cream for severe inflammation.
Warm (but not hot) sitz baths are a traditional therapy for piles: sit in about 8 cm of warm water for 15 minutes, several times a day, especially after a bowel movement.
Painkillers, such as paracetamol, can help relieve pain caused by piles. Products with local anaesthetic may be prescribed to treat painful haemorrhoids.
If you are constipated, a GP may recommend using a laxative.
However, these treatments do not get rid of the haemorrhoids themselves.
If you are pregnant, discuss any treatment, including dietary changes, with your doctor before proceeding.
If symptoms persist, your doctor may suggest one of the following procedures. Many can be performed as a day-case:
Injection or sclerotherapy. An internal haemorrhoid can be injected with a solution that creates a scar and closes off the haemorrhoid. The injection will only hurt a little.
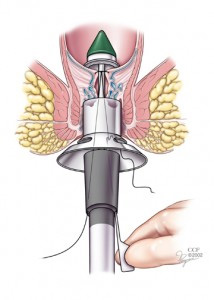
Banding. Prolapsed haemorrhoids are often removed using rubber-band ligation. A special tool secures a tiny rubber band around the haemorrhoid, shutting off its blood supply almost instantly. Within a week, the haemorrhoid shrivels and falls off.
Coagulation or cauterisation. Using either an electric probe, a laser beam, or an infrared light, a tiny burn painlessly seals the end of the haemorrhoid, causing it to close off and shrink. This is most useful for prolapsed haemorrhoids.
Surgery. For large internal haemorrhoids or extremely uncomfortable external haemorrhoids (such as thrombosed haemorrhoids that are too painful to live with), your doctor may choose traditional surgery, called haemorrhoidectomy.
The success rate for haemorrhoid removal approaches 95%, but unless dietary and lifestyle changes are made, haemorrhoids may recur.
You can prevent constipation by following a high-fibre diet. Meals and snacks should consist primarily of vegetables, fruit, nuts, and whole grains, and as few processed foods and meats as possible. If this is a big change for you, introduce the new foods slowly, to avoid wind.
If you aren’t able to eat enough high-fibre food, supplement your diet with stool softeners or bulk-forming agents. (Avoid laxatives, which may cause diarrhoea that can further irritate the swollen veins.)
Drink at least eight glasses of water each day; if your life is especially active or you live in a hot climate, you will need more.
Monitor your salt intake. Excess salt in the diet causes fluid retention, which means swelling in all veins, including haemorrhoids.

Hemorrhoid prevention hinges on a few key factors: diet, exercise, and bowel habits. A fiber-rich diet and regular exercise contribute to a healthy weight and reduce the risk of constipation, both of which can lead to hemorrhoids. Exercise also improves muscle tone, providing better support. When it comes to bowel habits, don’t ignore the urge to go, keep toilet visits short (under five minutes), and absolutely avoid straining.